It is a proud moment when you finally get a paper published that you have been working on for several months. I am always bemused by the amount of people on Social Media that like to criticize anything and everything the minute it is published. I ponder if these people have every written and submitted anything to a journal for publication and have gone through the sometimes months of formulating an idea, structure , content, references and writing and rewriting of an actual paper?
I was inspired to write this blog after having “our” paper published yesterday.
Let me take you on the journey of the “evolution “ of writing this paper.
In early November 2023 Giacomo (one of the papers coauthors) contacted me and the other authors to see if we would be interested in collaborating on a paper on the subject of nocebo and the health organization? I agreed immediately and began researching papers in the subject area. Surprisingly there were no specific papers on the subject, but several on related topics of issues poor communication and lack of respecting a patients’ beliefs and expectations.
Our group met via zoom for a discussion and planning meeting in mid November and we set up a google share format online. The four of us (another author would join later) set out working on ideas and a framework for a paper.
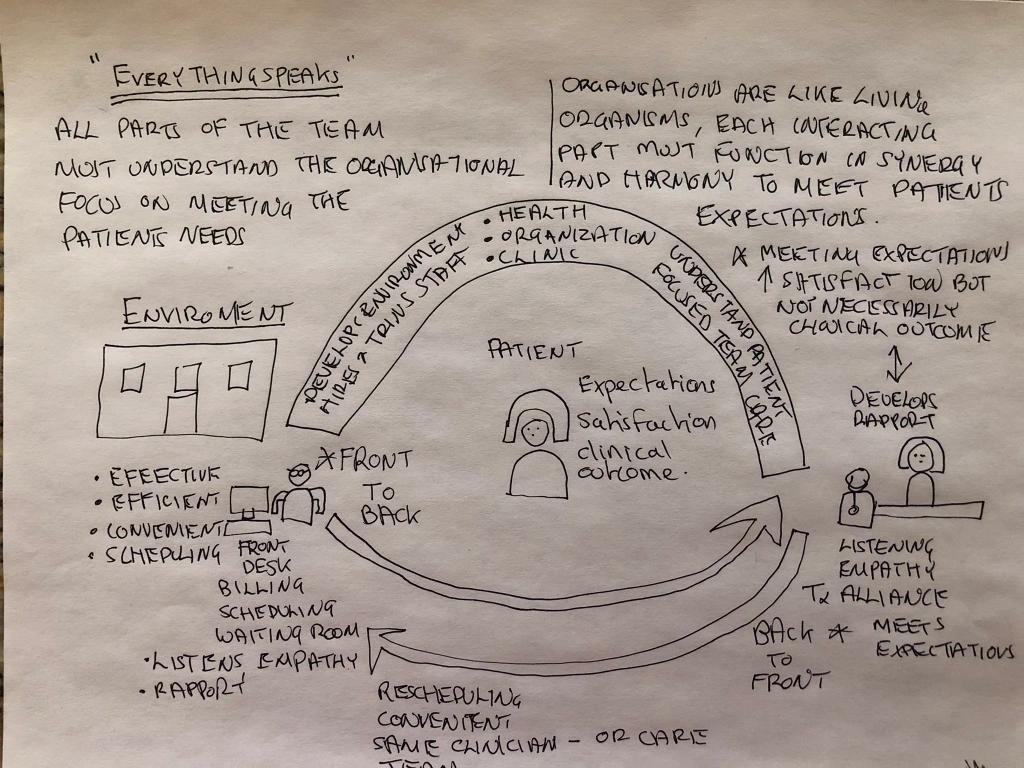
I do all my creative thinking on my afternoon cycle rides, so the afternoon after our first zoom meeting I set to work on an idea framework for our paper. On arriving home after a nice 2 hour cycle I sat down and sketched out my idea and frame work to present to the team at our next bi-weekly zoom meeting and shared on google drive.
First draft idea for the paper
Over the next day or so whilst cycling, after reading papers around the subject I sketched out another plan format.
More ideas
The group decided that we would use the ideas as a frame work for our paper. More ideas followed and were refined, but the sketches stimulated us to decide on a formal paper structure.
Over several zoom meeting we decided to allocate the sections to each individual to write and then place in the pig picture format. Over the next three months we each worked on separate sections, then we would incorporate the sections. Just before Christmas two of the team worked on the papers introduction and presented to the group.
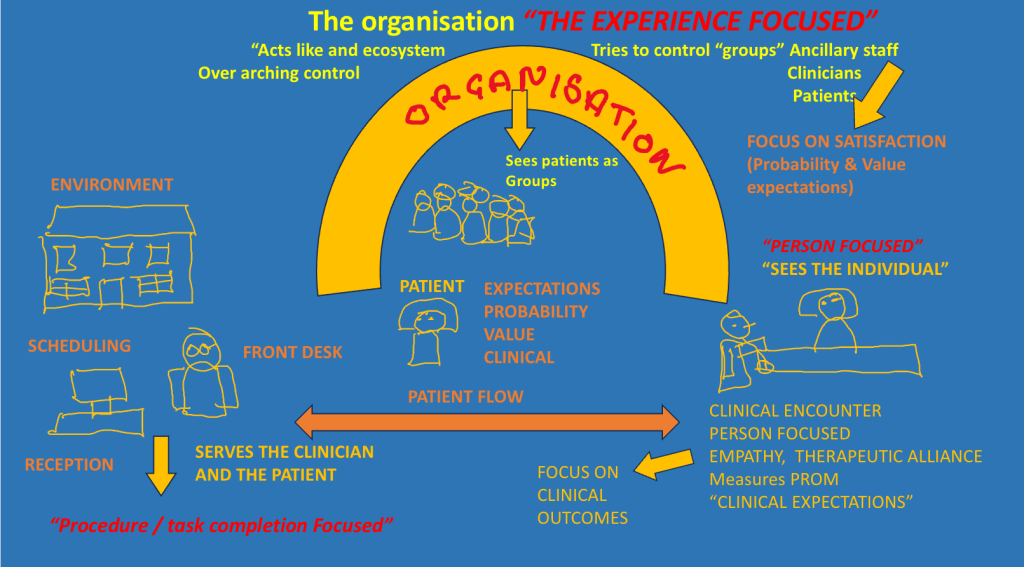
I worked on the figure and with feedback and discussions we had numerous iterations before reaching our final figure. I think that it is important for people to realize how many stages the creative process goes though before seeing what is relevant and published. Below shows the pictorial evolution of our final figure.
The final published figure.
As our article developed so did our thoughts around the figure. The article itself had many iterations , edits, format changes and updates. The final article took four months plus to write as a group. We sent the final article to some respected colleagues for review and suggestions prior to submission the the journal. We received mixed reviews and acted on some of the feedback.
After submission to the journal, we received several comments from the two reviewers. We met as a group via zoom and email, to address the concerns and update our paper. Our paper went through it’s final iteration and was accepted.
This paper took nearly six months from conception of an idea and frame work to publication. With five people actively reading, researching and sharing ideas, writing, editing and reviewing. It behooves all those who comment negatively about papers because they challenge a bias, to think about the work that goes into what appear to be a simple short paper. A lot of hard work goes into most if not all published papers.
I think that most authors are glad and relieved to see their hard work born into the world after months of hard work.
So a simple request, next time you read a new paper, spend a moment to reflect on the work that went into the paper and provide your feedback in a constructive manner, remembering the authors have gone through peer review and months of iterations prior to your comments.
Thanks as always for reading and a massive thanks to Giacomo, Maxi, Jerry and Alvisa, without your hard work dedication and effort, none of this would have been possible.
When we talk about pain we often discuss two terms, pain threshold and paint tolerance. Pain threshold simply put it the point when a stimulus is registered as painful (yes I do know the difference between nociception and pain) Pain tolerance simply put is measured as the intensity of pain which an individual can withstand before it becomes unbearable. It may include lower level intensity, but with a time factor in some, reflected by statements like “I can’t stand this any longer.”
I will propose that there is often confusion in patients and clinicians regarding the two terms and how treatment and exercise affect the two.
Patients often proudly report that they can put up with a lot of pain because they have a high pain threshold. Of course they are really talking about tolerating pain and hence referring to pain tolerance. I have to admit that I have frequently reported on twitter that I am totally intolerant to pain, I would prefer to have none. That withstanding if push comes to shove I do have quite a good tolerance if necessary and in context. The context is usually during endurance exercise when I know that the pain will eventually end. I am less tolerant of pain when I have no understanding of the end point, like when I burnt my hand.(Thread link here )
Clinicians often confuse the reason that patients are doing exercises. It is often reported on SoMe that patinet can exercise in pain and this will increase tolerance and allow them to be more resilient. I think we are confusing tolerance and threshold. If we look at tendinopathy treatment we often try to increase loading progressively as pain decreases with lower loads. This is not an increased tolerance this is in fact an increased pain threshold, ie heavier loads are require to produce a pain response. A recent paper discussed this and showed people with asymptomatic tendinopathy findings had higher pain thresholds. It is logical to extrapolate this to loading treatment response. Desensitization means higher pain thresholds. ( study link Here )
So in conclusion patients often confuse threshold for tolerance and therapist often confuse tolerance changes for threshold changes.
I personally am still intolerant to pain, I prefer not to have it, but I do tolerate pain in context when performing as an endurance athlete. I can tolerate pain of high intensity as long as I know there is an end point.
I haven’t written a micro blog for sometime and “pain” has been on my mind for awhile, so this blog is about what I believe to be, the confusion around the term “chronic pain.”
So what is chronic pain? (Take a moment to reflect on that question)
The reason I ask, what seems to be such a straight forward question, is that I believe that the answer will not be universal or straight forward.
I like to play on SoMe especially twitter (yep I know it’s now X but t will always be twitter to me.) there seems to be many interpretations of what chronic pain means, both amongst clinicians and lay people.
“The word “chronic” comes from the Greek word “khronikos,” which means “of time” or “related to time.” In medical terminology, “chronic” is used to describe a condition or illness that persists over an extended period, as opposed to acute conditions that are of shorter duration. The term emphasizes the prolonged or long-lasting nature of the condition.” (This is what ChatGPT answered to the question “what is the etymology of the word Chronic?”)
Chronic pain has been describe as any pain lasting beyond 12 weeks. This definition allows so many interpretations of what we mean by chronic pain. I think many clinicians just fill in their own gaps and often project this onto patients.
Chronic pain does not necessarily mean any of the following, constant, severe, ever present, lacks a heartbeat, never stops, there very single day, can’t be treated, won’t ever go away.
The reality of the term “chronic pain” is that it is literally a time label and not really a descriptor of how pain behaves, or it’s frequency, duration, intensity, distribution or how it responds to activity, medication or other treatments.
The time frame needs to be questioned too, there is more the so called “chronic pain” than lasting beyond 12 weeks. I personally experience pain on a daily basis, have done for years, none of my pains that I experience are chronic, in the medical sense. I am an avid cyclist and workout every single day with very rare exceptions. I feel exertion pain and muscle pains every day especially if I’m climbing, which is most days. I experience terrible pain on my Minnesota winter rides due to the extreme cold. The reason why none of these pains are chronic, is because I understand their onset, they are short lived and “normal” for the activities I perform, even though I’m 64.
I lasted ChatGPT and it came up with a similar answer: “In the context of sports training, experiencing daily exertion or muscle soreness for months may be more related to the physical demands of your training regimen rather than chronic pain in a pathological sense. Athletes often encounter persistent muscle soreness, fatigue, and discomfort during intensive training periods.
However, it’s crucial to differentiate between the normal discomfort associated with training and any pain that could indicate an injury or overtraining. If you have concerns about the nature of your pain or if it’s impacting your performance, it’s advisable to consult with a sports medicine professional or a healthcare provider. They can help assess whether the pain is within the expected range for your training or if there’s an underlying issue that needs attention.”
I propose that we need to seek to understand the person who is presenting with their persisting pain, (a term I much prefer) we need to seek to understand the onset, mechanism and nature of their pain, not just that it’s persisted beyond 12 weeks.
Everyone’s pain will be different but I assure you everyone’s pain will have a heart beat, no one has a flatlined pain that is constant and un fluctuating
pain has a heart beat.
So I now ask “what is chronic pain?” (Any different thoughts?)
There are a plethora of studies in the literature on providing education to patients to help reduce their pain, decrease kinesiophobia and increase self efficacy. Most of the studies provide what has been coined “Pain Neuroscience Education” or PNE, which comes in various content forms, but is predominantly a lecture based delivery. There has been a recent trend of suggesting that PNE is a stand alone treatment.
So I ask the question again in regards to PNE, are we confusing education with learning?
I will propose that for something to be effective education it has to have a positive learning effect on the recipient. A recent review suggested that most PNE studies deliver lecture based education, but do not measure what learning has taken place ( here )
A new study (in press here )has even tried to decide what “dose” of PNE would be most effective, again without discussing if any effective learning has taken part on the part of the recipient?
Maybe rather than trying to assess what length of PNE lecture has a positive effect we should be looking at which method and what type of deliver allows the best learning outcome?
Why is no one measuring what the participants involved in PNE are learning, or if they are learning anything?
We already know that PNE lectures have no different effect on pain compared to a placebo education program. ( here )
If education is effective then participants should be learning, lecture based delivery may not be the best way to enhance effective learning. There are various ways of testing if learning is taking place and whether the material learnt can be understood, utilized and applied. The teach back method is a commonly used method in clinical practice and education. (Here )
It may be time to stop taking about PNE and start talking about what people learn and if this has an effect on their pain, kinesiophobia and self efficacy. After all the intent of all education is for the recipient to learn something. Learning is the conduit to behavior change, without it there will be no change. It is also important to remember that people are also unlearning at the same time as learning, both sides of this learning experience must also take place for behaviors to change.
So a proposal, maybe we should be focusing on “Pain Neuroscience Learning” PNL rather than PN,measuring what has been learnt and the effect of this on the pain, kinesiophobia and self efficacy. Unlearning and learning are the intent of all education, shouldn’t we be measuring it before making outcome and causation statements?
Thanks for reading this micro blog.
Update after a nice evening cycle: link to 4 threads on X the artist formerly know as Twitter
In an older blog I posed the question “are we better than placebo?” Basically I was asking are we as practicing caring clinicians better than the sum of all the contextual non specific effects that surround our clinical interactions?
After a few days of interacting on twitter around a post on cupping, where I suggested the effects of this intervention are nothing beyond the theatric contextual placebo effects, I now pose the question “does it matter what we do as long as our patients report they are better?”
The black box of nonspecific treatment effects
I have long proposed that it is impossible to take the nonspecific effects out of so called “active treatments” and it is also hard to actually measure and separate out what the active effects are in many MSK interventions.
So back to the question does it matter what we do?
Things to consider:
As clinicians are we being open and honest about the interventions we use?
Do we understand the evidence around the effects and lack of effects around the interventions we provide?
Do the interventions we provide add value?
Are the interventions we provide safe with low harm profiles?
Should we be providing open label contextual placebos?
As clinicians are we imposing our beliefs on our patients?
As clinicians are we aware of the factors that influence clinical outcomes and patients reporting of feeling better?
highlights some of the issues and why ineffective treatments appear to work.
So does it matter what we do?
I think that each individual clinician has to answer this question based on their practice and patient population.
My bias is to be person focused and provide education and interventions to allow self care and recovery, avoiding interventions that may promote dependency on an intervention or an individual clinician.
We continue to be faced with the treatment conundrum “everything works for someone, nothing works for everyone”
So does it matter what we do? I proposed yes it does. We should be advocates for the truth and provide interventions in an open and honest manner without deception.
Remember it’s easy to be fooled as Feynman pointed out.
May 10th 2023 was a Wednesday and seemed just like any normal day. I had just arrived at our house in Brittany France and was a bit jet lagged even after a good nights sleep. At around 2pm I received a text from my wife in the US telling me to call my brother in Portugal. One of our friend, who we dog sit for, had been at the local hospital in Caldas, remarkably and coincidentally her husband was at the hospital for a follow up CT scan after a full in which he banged his head. My brother’s wife Chinye was rushed into the CT room for an emergency scan, in front of him. The message was brief and alls that I knew was that something had happened with a treadmill at the gym and Chinye had apparently passed out and hit her head. The reality of the situation was far worse.
I texted my brother and he replied that Chinye has passed out on the treadmill at the gym and banged her head and they were doing an emergency CT. He texted me some minute later saying they had asked him a few questions about headaches prior to the fall and rushed her back in for a second CT.
The next message I received was that Chinye was being rushed to the Lisbon neurosurgery hospital by ambulance. My brother was following closely in his car. Chinye was admitted to the intensive care of the neurosurgery unit. The head nurse informed my brother that they suspected that she had actually had a ruptured aneurysm that had caused her to blackout on the treadmill leading to the fall and banging of her head. The chief neurosurgeon had seen Chinye and reviewed her scans and had scheduled a craniotomy for immediately next morning.
Chinye in intensive care, still able to demonstrate her displeasure with the whole affair 😂
Next morning Chinye underwent the first neurosurgery on her brain. The surgeon preformed and open craniotomy drainage and clipping of the aneurysm. Thus began the next 4 weeks of recovery in the hospital and and eventual second surgery.
Day one post op
For the first few days after surgery Chinye slept for long periods of the day and night. The care was one on one nurse to patient care in the small neurosurgery post op observation ward.
This picture shows the large craniotomy incision and clips
Thankfully the surgery had been a success, over the next several weeks Chinye spent most of her days resting and sleeping. My brother with the aid and assistance of friends spent his afternoons traveling to Lisbon a good hours drive to visit in the late afternoon and evening everyday. The pattern of daily visits would continue for four weeks as Chinye recovered from her surgery.
By the first week of June it was decided that Chinye was ready to start early walking and getting up and down from the bed and chair. A few meters of walking with a frame left her exhausted and dizzy. The nurses persisted on a daily basis as the doctor wanted to get her ready for discharge to home.
Chinye up and about on her walker.
During the third week stay Chinye was transferred to a regular post op neurosurgery ward. She was being prepared for discharge. She underwent several follow up CT scans and on June 5th the lead surgeon decided that Chinye had persisting mild hydrocephalus and discussed inserting a drain from the brain to her abdomen to control this. Next day Chinye went into surgery to have a drain inserted one the left side of her brain. To add insult to injury she now had a new incision on the left side of her head and an abdominal incision. Surprisingly next day the nurses announced that it would be fine for Chinye to go home now the drain was in situ.
Next day my brother arrived at the hospital to bring her home. Lets say this was the start of more drama. Mark (my brother) and Chinye made it down in the lift (elevator) to the lobby, before Chinye became ill, he eyes rolling into her head and complaining of severe headache and nausea. Mark took her straight back to the ward, and after a heated debate she was readmitted.
Chinye remained a further few days in hospital. The doctor thought that the pressure changes in the lift may have cause the issue, but wasn’t sure. It was decided that Chinye would be discharged home via and ambulance so that she could be kept under observation. After a minor hiccup where the ambulance did not arrive to transport her, she finally arrived home on June 11th exactly five weeks post incident.
Chinye arriving home.
So Chinye was home. Let’s take a sidebar and review the enormity of the past month. My sister in law, came close to losing her life, thankfully saved by being in a public place with immediate help and access to the local hospital. She had access to a CT scanner and alert doctors who transferred her immediately to the neurosurgical hospital in Lisbon. She was lucky to have a great surgeon and follow up care.
Over the 4 weeks in hospital very little seemed to have been screened regarding her mental state, possible deficits both physical and neuro-cognitively. The main concern was on maintaining life and recovering some general wellbeing. On discharge no one had tested Chinye’s neuro-cognitive function. During her time in hospital she had suffered several episodes of paranoia, and delusions as her recovering brain tried to make sense of the world. She was convinced that there were people she knew on TV and that my brother was constantly Gaslighting her about things in general. She had also lost the awareness of time passing and got very confused about time of day and general passage of time. The doctors assured my brother that all these things were normal and would settle, as the brain recovered.
My brother had moved a bed into the living room and slept on the floor on a mattress, next to Chinye for the next two weeks. He basically became her full time carer, assisting her with all her daily duties and tasks like showering and toileting, feeding and dressing. Chinye continued to slowly improve but still fatigued quickly and continued to sleep for long periods of the day. She was still using a frame to walk to and from the bathroom.
Chinye happy to be home and sporting a new scar from her drain placement.
As luck had it I was traveling to Serbia at the end of June to teach, so I offered to pop down to Portugal to assess Chinye and start some functional and cognitive rehab, whilst I was on that side of the pond. The doctor had ordered some PT locally, but apparently there was a long waiting list.
On Monday June 26th I flew into Lisbon to be met by my brother. And so began 11days of rehab
“Eleven days of rehab and the amazing neuroplastic brain”
The next eleven days were an educational experience for all of us. Chinye’s auntie had arrived a few days earlier and was there to cook some traditional Nigerian food to build Chinye back up, her weight had fallen to 48Kg and she was a shadow of her fit former self.
Day one of rehab was assessment day. After a thorough neuro exam, only general slight weak of the left leg was apparent, no deep tendon reflex issues or sensory deficits were detected. Chinye was basically weak and suffering mainly from disuse atrophy and general tiredness related to the recovering brain trauma. Neuro-cognitively was a different matter. I worked for over a year in neuro psychiatry early in my career, which was now to stand me in good stead. Chinye has a degree in chemistry and had spent a long career as a science teacher and head Principle of an inner London school. I was reminded of one of my favourite books “When the Air Hits Your Brain: Tales from Neurosurgery” by Frank Vertosik MD
Knowing my sister in law was extremely important , my cognitive screen focused on drawing a clock, simple maths , deduction 7 from 100 progressively and spatial awareness tasks. it was apparent from day one that even drawing a clock was a major struggle. She could not do simple maths.4×5 was impossible. I developed a simple physical rehab program starting with how to get in and out of the chair independently , walking to and from the bathroom without the frame and some simple lower limb chair exercises.
I must admit this initial process was quite emotionally draining. I called to mind another of my favourite authors Oliver Sacks and his great books. Chinye would constantly remind me of his book “The man who mistook his wife for a hat, and other clinical tales” (the value of reading great books)
As well as starting some basic rehab with Chinye I focus on getting my brother Mark out of the house for long afternoon walks. Prior to my arrival he hadn’t been out of the house.
The view on our afternoon walks
Over the next 10 days I would develop a rigid daily schedule. Rise early, make tea, descend tot he basement and spin cycle for my usual 3 hours whilst tweeting. Shower eat a light breakfast and commence 2-3 hours of rehab with Chinye. Next go for a short walk with Auntie to the beach and get a cuppa in one of the beach side cafes. Light lunch and watch the end of the Tour De France, late afternoon walk with Mark. return home, and cycle out and about up the many steep steep hills for a few hours, dinner and bed.
Chinye’s physical rehab was the most pleasing , watching her improve on basic tasks like stair ascending and descending, going from my old favourite “good to heaven, bad to hell” one step at a time, to reciprocal, to no holding on over the space of 4-6 days. Chinye and Mark’s bedroom is on the third floor, so mastering independent stairs was a must. I set a series of progressive lover limb exercises programs incorporating theraband and balance exercises. By the end of the first week, we were ready to venture out ofthe house into the big wide world of noise, stimulus and colour.
The neuro-cognitive work we did each day was fascinating for both of us, I marvelled as I watched her brain literally rewire it’s self in front of me. For the first few days Chinye struggled to be able to place the figures on a clock, I set simple but for her challenging tasks, like split a circle into quarters, place the numbers of a clock on each quarter. For some reason she fixated on 5 being on the first quarter, she even drew all the number from 1-5 in the first quarter of the clock, but suddenly on day three with a bit of gentle coaching a neurone connected and it was obvious to her it was 3 not 5 and from the moment on she could draw the clock face with all the numbers in the right place. She was also aware of her mistake and could not believe that she had been focused on 5 being on the quarter.
First clock
Insisting that 12-5 is correct
The day of neuronal connection, a perfect clock
Our neuro-cognitive rehab continued with various topics from Pythagorus theorem , Avagadros number , use of Pi for circle circumference and area, basic chemical formulas, basic times tables, how to calculate change and use money. it was an interesting journey of discovery and rewiring. For all intensive purposes Chinye now seems conversationally normal, her deficits of simple maths and spatial awareness are improving, but she still lacks her higher problem solving skills and science knowledge, hopefully this will return in time as the brain helps and remodels.
“It’s time to go outside and face the world “
First venture outdoors
On the Saturday morning of my first week July 1st 2023 Chinye ventured outside under her own steam for the first time since May 11th. We casually strolled down the hill to the main Street and back again. Over the next few day we would increase our distance, we would meet so many people on our walk who would stop and give Chinye a big hug, surprised and over joyed to see her up and out of the house
We even did squats in the town square 😊
As the days passed Chinye got stronger and stronger and more confident in her physical and mental abilities. By day 9 of rehab we had moved the single bed out of the living room and her and Mark had returned to their bedroom upstairs. Chinye was independently showering washing and dressing another do all her own daily self care. On day 11 we walked down to the beach and sat and had a drink before walking home. This was 7,457 steps, 10 days prior she had been barley able to shuffle to the bathroom on a walking frame.
Goal achieved
After 11 days of rehab my sister in law was starting to look more like her old self. There is still a lot of hard work and healing ahead. I am in no doubt that her rapid improvement was due to natural history , healing and an improvement in her self confidence and self efficacy. Her improved diet and emotional support from Auntie, Mark and myself all assisted the recovery.
Since my return home Chinye has continued to improve and set new goals , she is walking further and has been out for lunch with friends. Yesterday she achieved the goal I set of going shopping to the supermarket and handling money.
Another goal achieved
Reflecting on the 11 days of rehab I learnt so much from the process, it also reminded me that as physiotherapists we play and important role in facilitating peoples recovery. It is important that we do not sell ourselves short. As I echoed on twitter our role is to assist recovery. Our actions matter, yes they look like common sense, but common sense is an oxymoron and our interactions are often uncommon.
So onward to full recovery and thanks for caring enough to read this blog.
This week Chinye returned to the scene of the crime and visited the gym where this journey began.
I left a detailed rehab plan
As Chinye improves I send her updates and progressions to her program.
This week she has progressed to a hilly walk circuit with Mark and continues to make great progress. The power of the healing brain. 😊
Climbing up to a great view. Onward and upward
Update Tuesday July 18th four weeks into her rehab.
I’m currently in the Azores dog sitting, yep it’s a thing. It’s a great way to see new countries and get free accommodation in exchange for looking after peoples beloved pets.
Whilst on a long walk with the dogs, this afternoon, I did some reflecting on who I am where I’ve been and what I’m doing.
Walking the dogs alongside the sea front at Fenais de Luz, The Azores
2023 is a notable year in my life’s journey. I qualified as a clinician and began practicing 40 years ago in 1983, in a month I will turn 64, the same age as my father was when he died of cancer. My father’s death has had a profound effect on my career choices and life, he would have been 85 this year, and since his death I have chosen to live my life without looking back , only looking forward.
People often ask why I work out 4 hour + everyday and eat a healthy diet, why I am currently living a somewhat unconventional life and am I still working and practicing? Of course I’m often asked “are you retired?” (A question that I dislike intently)
For a man rapidly approaching 64 (d-day age for me) I am remarkably fit and healthy. as I mentioned I work out (mainly cycling) at-least 4 hours everyday (yep no rested days) i take zero medications for zero complaints. I have al my own fully functioning joints that all have great range of motion and strength. Some of this may also be due t genetics, not just lifestyle, which I accept, my 84 mum still had all her own joints working fully and freely up to her mental decline.
Am I retired? Plain and simple no. Do I dance to the beat of my own drum, YES 💯.
COVID did me a huge favour, it allowed me to start seeing patients, mentoring and presenting educational courses online. It also made me realise that I could do this from anywhere in the world (assuming I had a good wifi connection, the great french wifi scandal shall not be mentioned in detail 😂)
My Dad (age 64) , me and my niece. This was taken a few weeks before he passed from metastatic bladder cancer.
I have structured my life to allow me to live and not work unless i choose to and when I choose to. Don’t get me wrong I don’t have heaps of money, but I live a frugal and fulfilling life.
Am I retired? I’ve been in the Azores now two week, the day before I left I saw a patient online, I have been managing via messenger over the last two weeks. I have done two mentoring sessions to far and distant places. I have peer reviewed an article for a well known journal. I have put together a presentation for this coming week and will be sharing it with a set of PT students, it’s about my 40 year journey in PT. I have read numerous research articles and posted extensively on Twitter. And most important of all I have shared two weeks in paradise with my wife and two beautiful dogs.
Do “Myths” of low back pain exist among young Indian college-going adults with a history of low back pain? A cross-sectional study
I’ve printed at the San Diego Pain Summit on moving from a Patient centered to a Person Focused care model.
So nope I’m not retired I’m just not working a 9-5 rigid schedule or 12 hour days, or 7 days a week.
This is a picture of my class at School in 1981, we re first year fresh faced, students, with our whole learning and careers ahead of us. (And yes I have hair 😂, I’m back row last on the right facing the photo.)
So in 40 years what have I achieved and where have I been? That’s the topic of my talk this week, hence the reflective walk.
My life is weird compared to many peoples, but my life is just that “a life”, I ponder on the next few years as I pass my father’s age. I have no plans, no agenda, no vision for my future. After 64 my life is a new journey, I’m fit and healthy and ready to live in tribute to my father. I want to do the things he had planned to do.
Retirement is for people who haven’t lived life and then seem to expect it will all change when work stops (I know that’s not true for everyone), but my dad was always a “when I retire I’m going to………..” kind of guy.
Am I retired? Nope an I never intend to be.
Looking forward to what the future holds.
2023 bring it on, there is life to be lived. I shall endeavour to remain fit and healthy. I will continue to Tweet, mentor, see patients online, peer review articles , co author papers and studies, write blogs, teach courses (sparingly) and present online.
Thanks for putting up with my reflexions and thanks if you actually read this far.
I woke up this morning, stretched yawned and bam a sharp pain just below my right clavicle (collar bone). “Poop”, I thought and a few other choice words. one getting up I had what could best be described as a painful pulling under my right collar bone. I went about my morning duties, went down stairs, put the kettle on, fed the cats, cleaned the litter boxes, brewed my tea, grabbed my iPad and headed down to my spin bike in the cave of pleasure & pain, that is my basement. Set up my iPad on the spin bike and cleaned the litter boxes out I the basement.
As I sat spinning and scrawling I noticed my pain was worse when I used my right arm to reach across to my iPad.
Position of my iPad on my spin bike
I tested horizontal adduction (reaching across my chest right to left) and it was sharp and painful with some restriction in range. “Oh poop!” was this my AC joint? (the little joint between your shoulder blade and collar bone) I tried turning my neck and it was restricted to the right and gave me increased pain under mu collar bone.
“MY NECK WAS OUT!!!!!!!!!” well for all intensive purposes that’s what it felt like or even my neck and shoulder were both ”OUT?”
I sat back into cycling position and realised I had much less pain, I tried a few shoulder extensions, using the mills maneuver (look it up ) but emphasised extension of the shoulder. The pain was unaffected, maybe it wasn’t my shoulder, but it still hurt to reach across my body.
Mill’s maneuver
I continued to spin and then decided to fiddle at my neck end to see if I could ”Put it back in?” (i am joking, but maybe not?) I stayed in my cycling position and tried side bending to the right with my head and neck from a semi slouched position (I can hear every Mckenzie therapist on the planet gasping) In the side bent semi slouched position I had relief of my pain. I repeated the movement about 20-30 times and by the end the pain was almost gone. I retested my horizontal adduction and it was much improved. I had put my neck back in, yeh!
I cycled for three hours, occasionally doing a few side bends and testing if my arm movement hurt. when i ended my session I was pain free, well at-least under my collar bone, my butt was another tale.
I wrote this blog in my head whilst out cycling after lunch out in the state park. I relaised I hadn’t felt the pain or restriction since this morning. I did post a thread before going cycling on mechanism versus source of symptoms as I was pondering on my pain event.
So although if I was a lay person I would have bet my house my neck was ”out” as a clinician this is not my thought process. But that said it is easy to understand why people seek out care and treatment from someone to ”put their neck back in.”
The human body is complex and it is hard to explain pain events like the one I had this morning. I believe they are probably more common than we care to accept, and the reason why some people do have ”quick fixes.” Each profession has an explanation of model for these events, chiropractic subluxation, osteopathic lesion, Mulligan facet fixation, McKenzie Derangement, etc etc. In my simple mind and on previous courses I have labelled these event ”re-arrangement” (it’s amazing what a threatened law suit can do for innovative word play)
There are all sorts lay words for these events like a crick in my neck or back, a pulled or a wrenched back, but definitely the most common is the spine being “out.” My simple model of explanation for these sudden onset mechanical pain event, that seem to respond rapidly to manual technique or simple self treatment procedures is the stone in your shoe. You can be happily walking along and get a sharp pain, your heel keep hurting until you take action, which can be, wiggle your foot around, shake your foot, stamp your foot, take your shoe off and tap the shoe, all of them can seem to perform the quick fix and allow you to go back to pain free function. I also use the bend finger model as described in the thread.
Bodies are complex, strange stuff happens and ”quick fixes” do sometimes occur, but they are not putting stuff back in that was out, well maybe not.
For a long time I have had concerns about the loose terms we use in MSK examination such as ”I cleared the spine” or ”first I would rule out red flags”, these terms seem to suggest that a) this is actually possible & b) once done the clinician is confident and will rarely. if ever return to these things as possible contributors or concerns in the persons current presentation.
I propose this is an error in clinical reasoning, we should replace these terms with ”lowering the probability of XYZ” and in the case of red flags switch to trying to identify them rather than ”ruling them out” ,which is a nonsense term, adapted from utilizing sensitive tests to ”rule out condition”.
I propose that clinicians should reverse their paradigm and be trying to identify relevant red flags that increase the suspicion of a serious condition, rather than “ruling out” anything.
As for the term “I cleared XYZ” I propose we again utilize the same reasoning and propose, ”we lowered the probability of involvement” ie “after a thorough history and exam it was apparent that the probability of the shoulder pain originating from the neck was minimal” as opposed to ”I cleared the neck from the picture”
A personal journey through a foreign health care system (during a pandemic) as an advocate for my mum.
My mum, brother and me circa 1961
This is a blog that I have pondered on writing numerous times over the last year. It seems pertinent that it is the anniversary of the events I’m going to describe. I think this is partly a blog written to get things of may chest and move on from my anger, somewhat. It’s a story that began just over a year ago and describes what it’s like as a seasoned medical professional to become embroiled in an advocacy role for a relative in a foreign countries health care system.
In April of 2021 (in the midst of the global COVID pandemic) I received a message from my brother in Portugal that my elderly 83 year old mum had fallen at home and fracture her femur. He went on to say she had been admitted to the hospital and was going to have surgery next day. so not the best of news, but made worse by the fact I live in Minnesota, USA and my mum in Malta some 5250 miles away as the crow flies.
I contacted the hospital in Malta to try to find out what was going on an was informed my mum had undergone surgery and a nail and plate placed in he femur to stabilize the fracture, an was resting comfortably on the orthopedic ward.
What ensued next was the bureaucratic wrangling and red tape involved in getting permission to travel from the USA to Malta which had the USA on the COVID red list, which meant no US residents could enter Malta due to the pandemic. Luckily I have contacts in Malta who helped me navigate some of this, I got in touch with the Health Minister and applied for an entry permit on compassionate grounds. This process took 3 weeks to sort out, but finally got permission to travel to Malta, with some rules. I had to have two negative PCR COVID test and an Antigen test negative a week and 25 hours before flying. then on arrival I would have to be in quarantine isolation for 14 days and test negative on day 10 for my quarantine.
Great, so I booked my ticket via Amsterdam and headed to the airport. luckily my COVID tests were negative and I had all the paper work in order to enter Malta. BUT, I was refused boarding in Minneapolis because I didn’t have permission to transit in Amsterdam, which required different COVID documentation. I returned home with my tail between my legs.
So on returning home from the airport and after calming down, I received kind help from a Dutch twitter follower who gave me details of the government department in Amsterdam that could assist me in my transit application. I had to rebook all my flights and schedule a return flight via Rome as I was not allowed to transit back though Amsterdam as there were no connecting flights and Holland was also closed to US travelers other than transit.
One week later I returned to the airport after repeating my three COVID test routine. I had a slight hiccup solved by only having carry one luggage.
I landed in Malta after transiting through Amsterdam on May 15th, all my paper work and testing was in order and was health screened at Luqa Airport Malta and told to go immediately to my quarantine address and stay there for 14 days until contacted by the health authorities. I was also given a number to call to schedule a COVID test on day 10. this all seemed a bit bizarre as I was not instructed on how to get to my mum’s apartment to quarantine. Luckily a friend of my mother’s came to pick me up, I double masked, he had also done some shopping for me.
I arrived at my mothers apartment and had arranged with a friend to have a spin bike delivered so I could workout and maintain my sanity. It turned out to be a life saver. I ended up spending up to 8 hours a day spinning and watching the Giro D’Italia on TV.
Fourteen days is a long time to spend in a third story apartment, but I did have the internet and a great view
I passed my isolation time emailing and calling the hospital to try and find out details about how my mother was progressing and enquiring bout the rehab plan and future plans for assistance. Prior to her fall my mother lived alone in a third story apartment, with 30 steps and no lift (elevator). a small back story, in the November prior she had contracted COVID and was bed bound for several weeks, she became very frail and my brother had to fly in and take her to his home in Portugal to get care and recuperate. She had fully recovered and returned to Malta, at her request, in mid March.
I facetimed my mother to discuss with her how she was doing whilst I quarantined. She did not seem to be her normal self and found it difficult to answer my questions. She was adamant though she didn’t feel she wanted to return to her apartment as she was frightened of falling again.
Apart from the frustration and isolation, I was getting more and more distressed with the mixed communication from her care team, I talked to nurses, social workers and Physios, who all had different plans and messages for me, I was led to believe my mum would transition to the rehab hospital so she could be able to negotiate her stairs before being sent home. This plan seemed to change on a daily basis. Six days into my stay I received a call from the lead ward physio saying my mum was ready for discharge home? I asked if he had assessed her ability to climb stairs and informed him she had 30 up and down and no lift. He relied ”no, but he would try her on stairs the next time he saw her.” It was a bizarre discussion even after I informed him that i was an experienced ortho physio as well as a son? I would later come to realize that my mum was on the acute orthopeadic ward and that they wanted the bed for other acute surgical admissions.
After taking with the Physio I called the social worker and ward sister and informed them that my mother could not come home for several reasons, 1. I was in isolation and quarantined in her apartment, 2. She needed to be abe to negotiate 30 steps, up and down and 3. She would need nursing care and a full time support as on Facetiming her it was apparent she was catheterised. They agreed she would be kept on the ward until i could visit in person.
I started to realize that there was going to be a ot of work to do to make sure my mother was safe to come home and that she got the appropriate care and rehab.
Let me tell you 14 days is a long time to be o your own with minimal food, I did order some takeaways and got them left outside for me to pick up once the delivery guy had gone.
On day 10 I was allowed to drive myself to the government COVID tests center , luckily my test was negative but I still had to quarantine for the full 14 days
There were some moments of beauty during my isolation
On May 29th 2021 at noon I officially ended my quarantine. I took a long walk on the beach and enjoyed a burger at the local restaurant.
May 30th would be my first visit to see my mum. She was in the acute orthopedic ward of the National Mater Dei hospital, due to COVID regulations visiting was restricted to one person and for one hour a day. OMG I arrived early and spent the next 30 minutes looking for a parking spot in the underground parking garage, it appeared every man and his dog were visiting, this would be a daily occurrence as everyone had to visit in the restricted time window due to COVID.
Mater Dei hospital was absolutely enormous, it is the biggest general hospital in Malta. I had flashbacks to my days working in UK hospitals as I navigated my way through the corridors to find my mothers ward on the third floor, the smell always brings back memories of my time in North Tees general hospital during my residency year.
I eventually found my mum and had a tearful first reunion. It only took my a brief interaction with her to realize she was not her self, she seemed vague and somewhat confused. She had a walker by her chair and she was sat with her now surgically repaired eg straight on a stool for support. I asked if she was doing exercises and walking, she replied ”only walking, no exercises” She was catheterized and in an adult diaper as she reported she wasn’t allowed to walk to the toilet on her own. My formerly healthy, active , independent 83 year old mum was now a frail, immobile, diapered, catheterized “old woman?”
After a chat we went for a walk using her frame, she had an extremely stiff knee with approximately 30 degrees of flexion, her leg was oedematous, and she shuffled rather than walked. I tried to hide my distress with the whole situation. The hour passed quickly and before leaving the ward I went to the nurses station, to find 6 or 7 nurses all sat on their phones scrolling. I explained who i was and asked for a meeting with my mums care team. The staff nurse said she would talk to the sister and I should come back tomorrow to see what was happening.
I wandered my way back to the car, where I sat and cried for a good 10 minutes.
Little did I know that over the next few days I would cry a lot an have many bizarre encounters with my mother’s health care team and fellow health care professionals .
Next day I arrived early to play find the parking spot with the rest of the population of Malta, or so it seemed. it didn’t help that the hospital was also the national COVID vaccination center.
10am and I entered the ward, as I was passing the desk the nurse waved at me an said that my mother’s care team would be rounding tomorrow at 9am and could i join them to discuss my mum’s care plan. I felt a little easier and went to see my mum and walk with her. Note I said ”walk with her” I am not a fan of PTs saying to patients ”i’ve come to take you for a walk” these are people not pets, as health care providers we walk with a person not take them for a walk.
Anyway, a much less stressful visit and I left after the allotted hour to shop for food and enjoy an afternoon of freedom in the Malteses sun.
For anyone who hasn’t been to Malta it’s a tiny island in the Mediterranean, problem is the population is 514,564 (I just googled it) and there are over 400,000 cars (I googled that too) the roads are narrow and poor quality and everyman and his dog (I think I’ve used that already) seems to be out and about during morning rush hour , lunch time and early evening. Let’s just say that driving in Malta is an experience to behold and made worse by driving on the left hand side of the road, when I predominantly drive on the right at home in the US (I did learn to drive in the UK so I am familiar with the process)
Next day I arrived early at the hospital for the ward round. My mum’s Maltese male friend (86 year old boyfriend) also join us, at my request. The clinical team consisted of two Doctors from the surgical ”firm” two OTs, two PTs, one nurse and a hospital social worker assigned to my mother. The rounds reminded me of my early days in the UK when I would do morning rounds with the surgeons, on the medical and surgical wards. The lead doctor discussed my mums surgery and her progress and the team each told us their thoughts. I then got a chance to talk after listening to them all. I explained I was only there from the US for a few weeks to get my mum safe and settled, I explained her situation prior to falling and also explained that she was frightened of going home to 30 steps and feared falling again. the discussion seemed productive and it appeared that the plan would be to send my mum to the rehab hospital to get her fit to go home with social care and a daily nurse. after the rounds ended the social worker gave me a list of private companies that specialized in live in care assistants, it apparently I was now in charge of organizing this?
I chatted with my mum and her friend and it seemed we had a plan.
I left after visiting time feeling more optimistic, by the time I got home to the apartment I had received an email from the lead doctor stating that the team had met and decided my mum would be discharged home at the end of the week. WTF, I had just met with them and decided on a plan which apparently had changed during my drive home. I contacted the social worker and asked to meet with her. She arranged for me to meet at 9am next day and had arranged another meeting with the care team. By that evening I was spitting feathers I was that angry. Spin David Spin.
Next morning I met with the social worker who apparently was as shocked as I was at the change in plan, she relayed that she had not been consulted either. I discussed with social worker my concerns that my mother appeared to be having cognitive difficulties and appeared to be in the early stages of dementia, the social worker said that none of the medical team had noted this. I explained that I thought she was not fit to make her own care decisions and that she was terrified at being sent home. after our meeting we walked to the ward, where we were met, at the nurses station, by yesterdays care team plus a new lead male PT and the ward sister. We stood in the ward corridor and the sister began by saying that my mum was doing well and was ready for discharge? I asked how they though she would navigate 30 stairs on a walker shuffling ?The male PT piped up ”she did stairs with me this morning” I asked “how many?” he replied 15, I ask how he thought 15 was 30 and that this was unacceptable. The PT then became passive aggressive and told me she could sit on a chair half way up and rest. Let’s just say the next few minutes of interaction where not my proudest moments, but I feel where necessary, I informed one and all gathered that this meeting was totally inappropriate being held in a ward corridor in public view, with no privacy with basically 12 care staff trying to tell a patients son that he was wrong and that his mother was just going to be discharged. I also informed them that i was uncomfortable with their attitude and that they agreed on a plan the day before and changed it without discussing why with me. The tipping point for me was when the PT asked if my mum was “even”Maltese. (luckily she is she was naturalized on her 80th birthday)
I relayed to the care team that I also felt my mother was having cognitive issues and requested an assessment be done to evaluate her decision making abilities. after everyone calmed down the ward sister agreed and decided that after the assessment we would decide my mother fate next day. What became apparent after the meeting was that the goal of the acute ortho team was to free up the wards beds for other surgical cases. my mother had become a victim of the system and of COVID as the doctor kept saying the longer she stays here the higher the risk of infection. I later discovered that the rehab hospital plan was also off the table due to the COVID pandemic.
I left the hospital feeling drained and I am not ashamed to say I drove to a local tourist spot and had a giant piece of chocolate cake to clam my nerves.
Little did I know that the next three days would be a roller coaster ride of emotions. I returned to the hospital next day and on arriving on the ward was informed they hadn’t assessed my mum’s cognitive abilities yet, but at the end of visiting time the doctor and the social woke wanted to discuss a discharge plan with my mum and I? yep a new plan an new day, bizarre. My mu and I went for a walk and did some exercises for her knee. at the end of visiting as previously announced the doctor and social worker arrived. they sat with my mum, her friend and I to review our options, discharge home with support organized by me and the social worker. My mum listened and then told them she wouldn’t go back to her apartment under any circumstances, her boy friend then chimed in and said she could live with him? OMG the fly in the proverbial ointment. I had to step in and explain that he lived with his son and daughter-in-law and that there was no spare bedroom, plus I would need to chat with them first. Another day another cluster F^*k. it became apparent they just wanted my mum off the ward.
That evening I visited my mum’s friend and his son at their house. long story short my mum was not relocating to their house. I don’t drink alcohol, but if i did this would have been a few whiskies evening. Spin David spin 🚴🏻
Next day was ground hog day, another meeting with my mum, the doctor and social worker. I explained that my mum moving to her friend’s house was a no go, they replayed my mum had been cognitively assessed and was fine to make decisions. (I protested and suggested their test was wrong, they didn’t listen, I tried to insist that I have a background in cognitive assessment and as her son was aware she had mental issues, no ne would listen.) The doctor tried to explain to my mum that she was to be discharged home, my mum just kept saying no and crying. Another day, and no decision or solution.
On returning home i wrote a long email to the social worker outlining my concerns regarding my mums care and long term plan, I asked for solutions other than returning home. She replied later that day informing me my mother was eligible for state nursing home care as she was a Maltese citizen. that evening I formulated a new plan to put to my mum.
After playing the parking lottery next morning, I returned to the ward and chatted to my mum whilst we walked. Remarkably she was starting to walk quite well despite her still stiff knee. I discussed going to a nursing home and she just listened. once again the doctor and the social worker appeared at the end of visiting. Today was D day, the doctor sat on the edge of the bed and asked me if i had discussed the options with my mum, I nodded in the affirmative.
The doctor asked my mum if she wanted to be discharged home, she teared up and said ”no”, the doctor said “great then the nursing home it is.” That was it that was how my mum was sent to a nursing home. That afternoon she was discharged from the ortho ward to a long term elderly medical ward to await a place at a state nursing home. Ortho ward team mission accomplished.
I drove home dismayed.
Over the next few days my mum became more and more confused, i discussed this with the new ward staff, they suggested it just part of being moved and her surgery, I knew it wasn’t.
It took four days and I received a phone call that a place had been found in a nursing facility and my mum would be transferred directly from the hospital. The nursing home was a lengthy drive away close to the airport. That afternoon I went to buy some toiletries and new nighties for my mum. I arrived at the new nursing home for the hour visiting time only to be told my US vaccination certificate wasn’t acceptable and i needed a Euro COVID pass, luckily I showed them all my government clearance paper work and they let me in.
My mum was sat in reception waiting for the facility doctor to assess her. The facility was clean and the staff seemed friendly and caring. My mum was extremely confused and thought that she was at my house in the US. (once again a sign of her declining mental status) she was assessed by the doctor and placed on some new meds. I met with the facility coordinator to discuss finances and such. the hour passed quickly.
Next day I returned to the new home feeling happy that my mum was now in a caring environment. OMG it was the day from hell, my mum was agitated, confused and didn’t want to stay in the home, she was verbally abusive to me and told me i had put her in a home so i could go home to the US. I calmed her down and walked with her. she seemed confused, but I put this down to the new facility and her mental status.
That lunch time I had arranged to meet a friend for lunch, it never happened.
I had a front wheel blow out in my mum’s old car, then of course the spare would not come out of the boot (trunk) and when it did it was flat. I had no phone and limped the car to the nearest garage. the man at the garage was lovely and fixed everything and gave me a place to wash up. I cried again.
Next day I visited mum she was more settled but very confused, she was walking around without her walker, she had forgotten she had had surgery. this was my last day, I spent my time explaining this to her, but she didn’t seem to register. on my way home I stopped to get another bloody COVID test so I could go home
I left Malta and my mum with a heavy heart, but knowing she was safe and being cared for, little did I know what the next dew months would bring.
A week after arriving home I received a message that my mum had fallen in the home and was back in hospital. She had another surgery that week as according to the doctor her femur fixation had failed. she stayed in the hospital a week and returned to the home to rehab (they had on site physio). I facetimed her regularly, she was becoming more confused.
At the end of July I got another message she was back in hospital after another fall, she had this time fractured her same femur at the knee. Another surgery, more rehab and a return a new nursing home. This home was the national dementia care home. My mum had developed obvious dementia, so obvious even the ortho staff were now aware of it.
My mum has been bed ridden since returning to the new home. I visited Malta again this year and she is safe, well cared for and doesn’t know who I am. She has developed expressive aphasia which is distressing to those that interact with her.
If you have made it this for, bless you. I don’t think i intended anyone to read this, but writing it all down has been healing.
I miss my mum, I weep for our medical systems and health care professionals who are caring but focus on the wrong things. I am an advocate for person focused care, not discharge drive care, I want people to be cared about not just cared for. As health care professional we can all do better.